THE AUTHOR:

Surgical risk indicators can be found in hospital data prior to a surgical procedure, but many health organizations fail to make quick, data-driven decisions. To build surgical risk prediction software, hospitals have to establish a cohesive system between EHRs, lab and test results, patient and clinical histories and notes, data on surgical procedures, and workflows both within and outside the surgical context.
The main obstacle is identifying risk signals within fragmented data. Increased risk may be evident within a patient’s prior admissions, lab results with flagged values, medication history and profile, procedure complexity, comorbidities, clinical notes, and patient age. However, the information is typically stored across multiple systems and is only assessed through manual review by care staff.
Not detecting and addressing risks leads to cancelled surgeries, extended patient hospitalizations, waste of valuable hospital resources, and creates unnecessary demand on already burdened clinical staff. Using advanced analytics to predict future trends and events is of growing interest in healthcare to identify and control risks and improve the responsiveness of organizations. It is predicted that the market for healthcare predictive analytics in the U.S. will grow from USD 7.2 billion in 2025 to USD 30.99 billion in 2035.
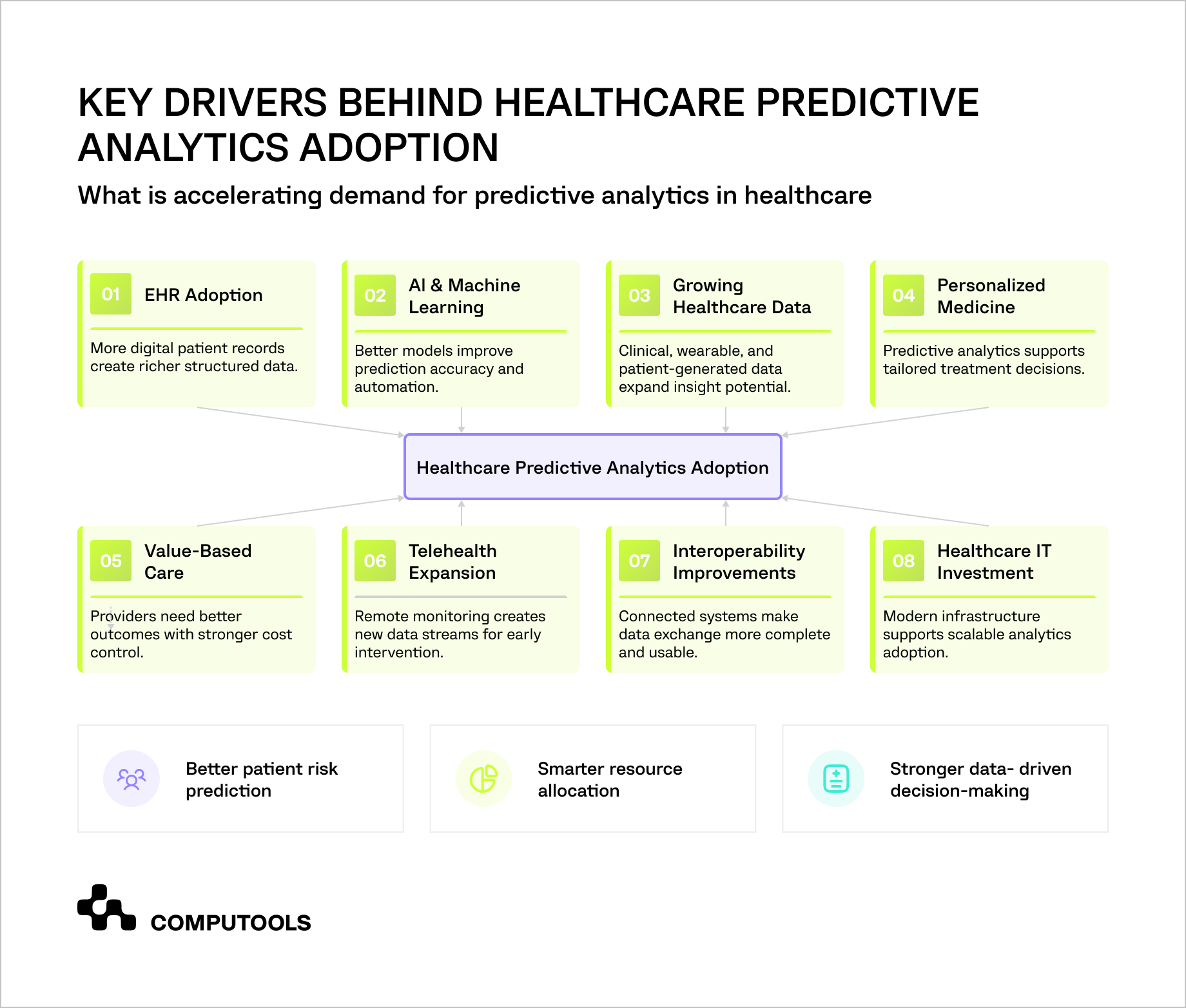
AI is beginning to change healthcare predictive analytics and the pattern of assessing surgical risks in hospitals. Studies show that surgical complications can potentially be predicted in advance by using AI and machine learning to assess the likelihood of encountering complications and to identify high-risk surgical patients. A study on AI in perioperative care found that machine learning techniques were superior to traditional methods of assessing surgical risk in the preoperative phase, thus identifying high-risk surgical patients.
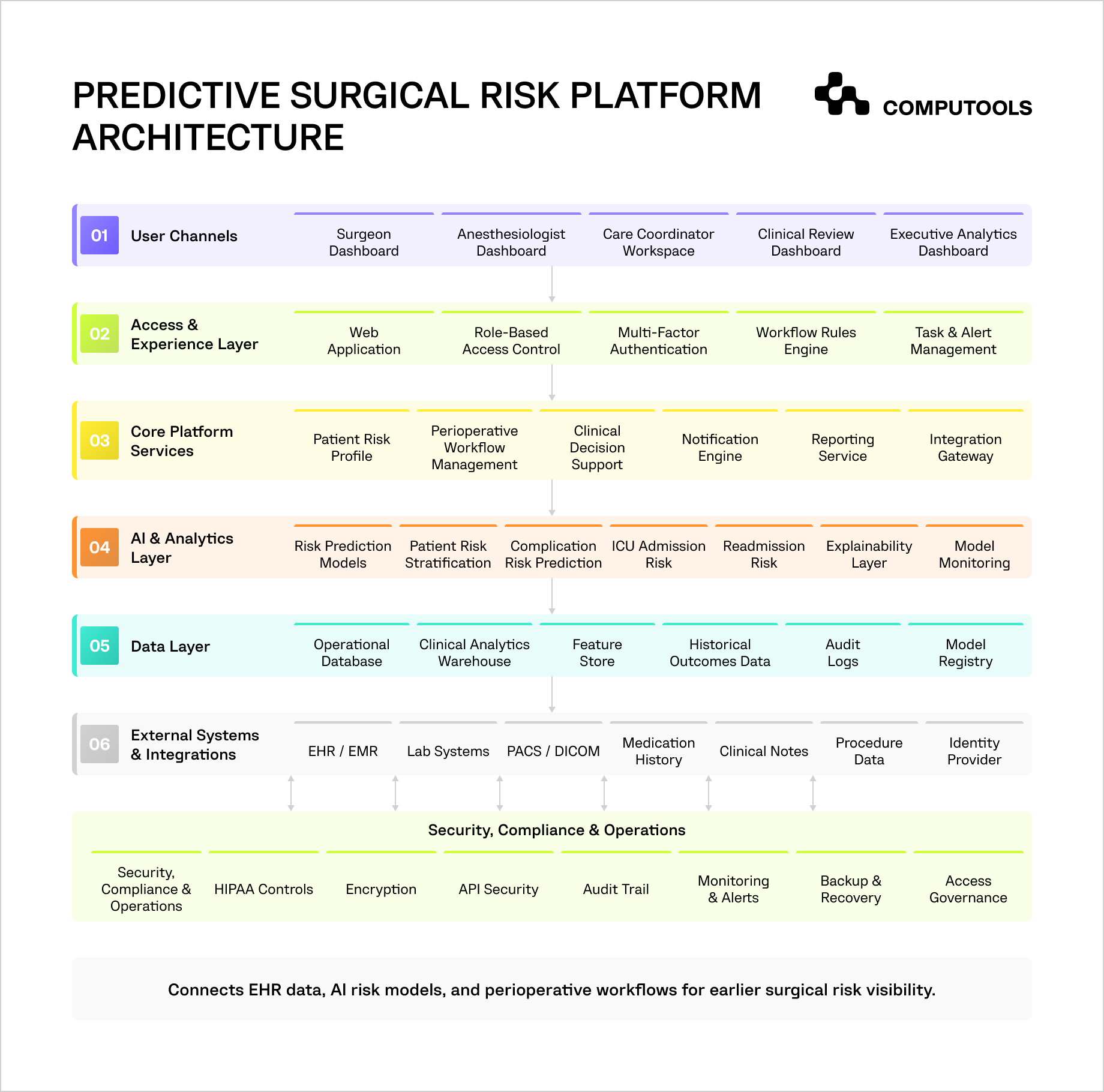
This article explains how to build a predictive surgical risk platform using EHR and clinical data, covering architecture decisions, data modeling, AI development, integrations, security requirements, workflow automation, and the steps needed to turn risk predictions into practical perioperative decisions.
Essential features of surgical risk prediction software
Clinical decision support software connects clinical data collection, AI risk modeling, and decision-support workflows, along with access control.
| Feature | What It Does | Business Value |
| EHR data integration | Gathers information concerning patient demographics, diagnoses, lab values, medication history, allergies, previous procedures, and clinical notes from the hospital systems. | Creates a more thorough understanding of surgical risk and decreases the need for time-consuming manual chart reviews. |
| Patient risk stratification | Groups patients by risk level based on clinical history, current condition, procedure type, and predicted outcomes. | Predicts the risk of several negative outcomes including post-operative complications, the need for admission to the ICU, unplanned readmissions, negative impacts of extended LOS, and risk of unplanned procedure cancellation. |
| AI surgical risk prediction | Estimates risks such as postoperative complications, ICU admission, readmission, extended length of stay, or cancellation risk. | Gives clinicians and administrators earlier visibility into high-risk cases. |
| Clinical decision support | Turns risk scores into alerts, recommendations, checklists, and next-step actions. | Moves risk insights into daily workflows instead of leaving them in reports. |
| Explainability layer | Shows which clinical factors influenced a patient’s risk score. | Builds clinician trust and supports safer use of AI-powered surgical risk assessment. |
| Perioperative workflow dashboard | Shows patient readiness, missing data, risk level, required reviews, and assigned actions. | Reduces coordination gaps between surgical, anesthesia, nursing, and admin teams. |
| Automation and alerts | Triggers notifications for missing labs, high-risk patients, incomplete pre-op steps, or required specialist review. | Reduces manual follow-up and prevents risk signals from being missed. |
| Model monitoring | Tracks model accuracy, drift, rejected recommendations, and performance across patient groups. | Keeps clinical risk prediction software reliable after launch. |
| Security and audit controls | Manages user roles, encryption, audit logs, API security, and access history. | Protects patient data and supports compliance, accountability, and operational trust. |
| Reporting and analytics | Tracks risk trends, high-risk case volume, complication patterns, and resource demand. | Gives executives clearer visibility into surgical risk, capacity planning, and operational performance. |
With these features, surgical teams gain risk visibility sooner, and hospital leaders understand the impact of risk on capacity, staff, and resources, as well as on perioperative outcomes.
Computools case study: SurgeryOps as a foundation for data-driven surgical risk visibility
Surgical risk prediction software depends on one thing before AI enters the picture: reliable clinical and operational data. If patient parameters, diagnostic inputs, doctor availability, room schedules, and procedure details sit in disconnected systems, hospitals cannot build accurate risk models or act on risk signals in time.
This was the core issue in the SurgeryOps project. Computools worked with a U.S. multi-specialty hospital performing 30–50 procedures per day. The hospital needed to replace fragmented preoperative coordination with a secure platform that could organize procedure planning, patient-related data, room allocation, and diagnostic information in one environment.
The main challenge was not only scheduling. It was data fragmentation. Staff had to coordinate procedures across spreadsheets, calendars, and separate internal tools, which increased planning errors, created room conflicts, and limited visibility into daily surgical readiness. For a predictive risk platform, the same fragmentation would lead to a more serious issue: a lack of patient context and insufficient inputs for AI surgical risk prediction.

Computools developed a centralized preoperative planning platform with ASP.NET Core, C#, React, Microsoft SQL Server, REST APIs, DICOM integration, role-based access control, encryption, and audit logging. The system brought order to the control of scheduling data, patient parameters, diagnostic assessments, workflows, user permissions, and operational changes.
The outcome was:
- manual planning time dropped by 60%;
- planning errors by 40%;
- scheduling conflicts and idle procedure rooms by 98%.
More importantly for this topic, the project shows what hospitals need before adding AI-powered risk assessment: clean data flows, traceable access, integrated diagnostic context, and workflow logic that supports action.
That foundation is essential because medical risk prediction does not add value as an isolated score. The system adds value when risk is identified, contributing factors are communicated, the appropriate team is notified, and the next step in the perioperative workflow is automated.
How to develop a surgical risk prediction software solution
To develop a predictive risk platform, healthcare administrators should focus on the system’s decisions that the platform needs to improve. The system should incorporate the ability to identify high-risk patients earlier, articulate the reasons for that risk, and appropriately direct the case to the right clinical team to support safer perioperative planning.
1. Define Which Surgical Risks the Platform Should Predict
Step one is determining risk scope. What is the platform designed to predict? Post-surgery complications? Perioperative risks? Post-op ICU admission? Post-op readmission? Post-op extended length of stay? Surgical site infections? Request for an anesthesia review? Cancellation risk? All the above?
This step is important because each risk category will require its own data set, model design, validation, and workflow. For example, the prediction for ICU admissions may depend on different factors than cancellation risk. Cancellation risk may depend on pre-op verifications and/or medical clearance, diagnostic results, insurance, lab tests, or even changes to the schedule.
Technically speaking, the prediction target needs to be defined. The product team needs to consider what a complication is, where and when it will be recorded, and how it will impact the model. Defining risk in broad or ambiguous terms will also make the platform hard to test and will undoubtedly reduce the platform’s trustworthiness to clinicians.
In practice, start with 2 to 3 risk categories that will bring the most value. Link each one to a clear action. For example, a high ICU risk score can trigger a bed planning review. A high readmission risk score can alert discharge planning teams. A high anesthesia risk score can route the case to preoperative review before the surgery date.
2. Build the Clinical Data Model Around EHR and Perioperative Data
AI-enabled surgical risk prediction depends on the quality of the clinical data model. The platform should not pull raw EHR data into a black box and expect reliable results. It needs structured, validated, and clinically meaningful data.
Useful inputs may include patient demographics, diagnoses, comorbidities, medication history, allergies, lab results, vital signs, prior admissions, procedure history, anesthesia notes, ASA class, imaging references, pre-op assessment data, discharge records, and postoperative outcomes.
The software architecture should separate the EHR as the system of record from the analytics layer used for risk modeling. The platform can use an operational database for current patient status, a clinical analytics warehouse for historical data, and a feature store for model-ready variables. This structure allows teams to score patients without overloading the EHR or mixing live workflow data with model training data.
Data quality rules are critical. The platform should validate units, remove duplicates, normalize codes, detect missing values, and track data lineage. If a lab value is missing, outdated, or recorded in the wrong unit, the system should not silently use it in a prediction.
SurgeryOps Insight
Computools used Microsoft SQL Server to store scheduling data, patient parameters, audit logs, and access rules. For a surgical risk prediction software, the same database discipline matters because risk models need traceable inputs, reliable patient context, and clean historical data before they can support medical risk prediction.
For organizations preparing their data foundation first, Computools’ guide on how to build a healthcare data platform explains how to structure healthcare data for analytics, reporting, and AI use cases.
3. Design EHR Integration for Surgical Risk Prediction
A predictive platform becomes useful when it works inside existing hospital workflows. That requires careful EHR integration..
The business question at hand is whether the platform will read EHR data only and return risk scores to the EHR, or if it will support two-way workflow actions (alerts, task creation, documentation updates, and changes to review statuses). Each of the three scenarios will impact compliance, user adoption, integration effort, and clinical accountability.
From a technical standpoint, the platform will require a combination of FHIR APIs, HL7 interfaces, REST APIs, integration of an identity provider, event-based triggers, data synchronization logic, and retry queues. The platform will also need comprehensive logging capabilities to track data access, scores, alerts, recommendations, overrides, and all workflow actions.
Risk scoring should occur at key clinical events. These may include the scheduling of a surgery, the completion of a pre-operative assessment, the arrival of new lab tests, a change in the history of medications, or the documentation of a change in the status of a patient by a clinician. This will ensure that teams work with the most current and relevant risk scores and will not act on outdated or stale information
If integration is weak, the system can create more work instead of reducing it. Staff may need to copy data manually, check two systems, or compare conflicting risk views. The platform should bring risk signals into the workflow where clinicians and coordinators already make decisions.
SurgeryOps Insight
Computools implemented REST APIs and DICOM integration to connect the platform with internal hospital systems and diagnostic imaging data. This same integration layer can support EHR integration for surgical risk prediction, lab data access, imaging references, and clinical data analytics.
4. Create the AI Risk Prediction Layer
After the data foundation and EHR integration are ready, the platform can turn clinical data into risk scores, explanations, and recommended actions.
The crucial question is what fits the use case the best – rule based logic, machine learning, large language models, or a hybrid model. For the majority of structured risk tasks, AI-powered surgical risk prediction requires the use of validated machine learning. Large language models may be useful for controlled tasks summarizing risk factors, analyzing clinical notes, or justifying patient flags.
From a technical perspective, this layer demands feature engineering, model training, calibration, validation, explainability, tuning thresholds, testing bias, and the monitoring of models. Only presenting a risk percentage isn’t enough to drive the adoption of the model. To build trust, clinicians should be able to see the primary risk score factors, the score confidence and the next step recommendation.
For example, the model may assess a patient to be at a high risk for developing postoperative complications due to a combination of prior lab results, past hospitalizations, current medication, the patient’s age, procedure, and pre-existing conditions. The interface should show these factors clearly so the care team can review the logic.
Production deployment should also be controlled. Each model version should have training data records, validation results, approval status, performance metrics, deployment date, and monitoring rules. If this layer is rushed, the platform may produce unreliable scores, increase alert fatigue, and weaken clinician trust.
For teams planning AI governance early, Computools’ guide on HIPAA-compliant AI architecture explains how to design protected data flows, model accountability, access control, and auditability for healthcare AI systems.
5. Turn Risk Scores Into Clinical Decision Support
Perioperative risk assessment software should convert risk scores into practical clinical and operational actions.
The key decision is what happens when the system identifies a high-risk patient. High complication risk may trigger a pre-op optimization checklist. High ICU admission risk may notify bed management and anesthesia teams. High readmission risk may involve discharge planning earlier. Missing lab results may create a task for the coordinator.
Technically, the clinical decision support layer should include risk category, contributing factors, recommended action, responsible user, escalation rule, due date, override option, and audit log. The system should record whether each recommendation was accepted, rejected, ignored, or overridden.
This feedback improves the product. If clinicians often reject a recommendation, the issue may be poor data quality, an incorrect threshold, unclear explanation, or workflow mismatch.
Alerts should be specific. “Patient is at high risk” is too vague. A stronger alert would say: “High ICU admission risk. Main factors: prior admission, abnormal creatinine, procedure type, and age. Recommended action: anesthesia review and bed planning check.”
If this step is ignored, the platform becomes passive clinical risk prediction software. It may identify risk, but it will not change how teams plan, communicate, or act before surgery.
SurgeryOps Insight
The platform used ASP.NET Core and C# to handle scheduling logic, doctor assignment, access control, conflict detection, and workload calculations. For predictive surgical risk software, similar backend logic can support risk recalculation, alert routing, patient risk stratification, and clinical decision support workflows.
6. Add Workflow Automation and Admin Controls
Predictive analytics in healthcare creates value when risk signals move to the right workflow without adding manual work.
The most critical choice here is which actions will be fully automated and which actions will require manual intervention. For example, the platform has the capability to fully automate missing-data notifications, risk recalculations, pre-operative checklists, task assignment, escalation notifications, and filtering patient cohorts. Deciding on the appropriate clinical pathway, however, will always need to remain in the hands of qualified personnel.
From a technical perspective, the platform will require a rules-based workflow system. At minimum, the system should be able to define when an action is to be performed, the recipients, the respondents, the deadline, the consequences for not meeting the deadline, and how the event is logged.
Changes should be easily made by administrators to include configuration of risk bands, setting a limit on score thresholds, and establishing department workflows, roles, and notification settings.
If a patient has an increased risk score, the platform automatically notifies the anesthesia department to review the updated score. If the recommendation is overridden, then the system should document this.
For example, if new lab results increase a patient’s risk score, the platform can recalculate the score, update the dashboard, notify the anesthesia team, and create a review task. If the clinician overrides the recommendation, the system should record the reason.
The right design automates routing, reminders, and visibility while keeping medical judgment with clinicians.
7. Build Security, Compliance, and Reliability Into the Platform
Security approach directly affects trust, continuity, compliance, and adoption in clinical risk prediction software.
The main consideration is how the platform will control access and protect data and, in turn, how this will impact the company’s risk exposure in terms of availability. A surgeon may need access to patient level risk details in relation to their assigned cases. An executive may need access to aggregated risk data. An IT admin may need unrestricted access to the platform without clinical decision making rights.
From a technical viewpoint, the platform should feature control access based on roles and attributes, encryption at rest and in transit, secure API authentication, a complete audit log for all system activities, session control, backup and recovery, system monitoring, and incident response alerts.
The platform should also allow for data minimization. Each individual should only be able to view the information required to perform their function. Leadership dashboards should be designed to focus on trends, capacity, and risk operational performance.
Reliability is equally important. If the platform is unavailable during pre-op review, teams may miss important risk signals or return to manual workarounds. The system should include health monitoring, logging, failover planning, backup policies, and recovery procedures.
SurgeryOps Insight
The project used RBAC, encryption, and audit logging to restrict access to patient data and track sensitive actions. Predictive surgical risk software needs this control because risk scores, clinical notes, patient parameters, AI explanations, and override history should follow different permission rules.
If the platform runs in the cloud, infrastructure security should be planned early. Computools’ guide on cloud security in healthcare covers the controls needed to protect connected healthcare systems, sensitive data, and cloud-based workloads.
8. Test the Platform With Clinical and Operational Scenarios
Testing should reflect real perioperative workflows, not only technical requirements.
Testing has to cover the full range of real-world workflows in the perioperative context, rather than focusing solely on the technical barriers.
Key decisions involve determining scenarios that need to be safeguarded before the system is launched, such as (but not limited to) the scheduling of high-risk patients, absences of lab values and an updated medication history, abnormal results, canceled procedures, urgent surgery, override of risk score, failure of EHR integration, and low confidence in the model.
Testing plans have to cover a wide scope of testing, such as unit and integration testing, as well as testing permissions, security, and data integrity, in addition to performance, workflow simulation, and user acceptance testing, as well as AI validation, calibration checks, and bias audits.
In this context, validation of AI will have to account for the issues of false positives and negatives, model drift, performance across patient groups, rejected recommendations, and alert fatigue. A model may perform well on historical data but fail when documentation patterns, procedure types, or patient populations change.
The platform should also be tested for speed and usability. Risk scores should load quickly. Alerts should be clear. Dashboards should show the highest-risk cases first. If the system feels slow or confusing, teams may stop using it.
Launch your predictive surgical risk platform within 1–3 months instead of years, with secure EHR integration, AI-ready clinical data pipelines, and a scalable architecture built for real-world healthcare.
Why choose Computools for surgical risk prediction software development
Hospitals need to connect EHR data, structure clinical records, protect patient information, support clinician workflows, and turn risk predictions into actions that reduce perioperative uncertainty.
Computools healthcare software development services tackle the full spectrum of a product’s needs. Our team examines clinical workflows and user roles, designs secure data flows, and engineers compliant software meeting the complexity of regulated healthcare environments. This is especially important when a platform needs to perform risk assessment, patient risk stratification, and clinical decision support, while avoiding extra burden on medical staff.
With hospital software development services, our company connects the platform with existing hospital systems, including EHR, EMR, PACS, DICOM, staff scheduling, billing, and reporting tools. These integrations help to eliminate duplicate data input, view risks in less fragmented ways, and provide an up-to-date context of the patient to the medical staff during pre-surgery.
Computools data engineering services address a key challenge of AI-backed surgical risk prediction – the preparation of clinical data for dependable use. We build data pipelines, align terminology, validate lab values, structure historical procedure data, and prepare datasets for advanced analytics. Risk models benefit from cleaner data, and hospital administrators receive more dependable reports.
On the AI development front, Computools builds the logic for risk prediction, recommendation workflows, explainability, and model monitoring. This supports AI-powered surgical risk assessment that clinicians can review, challenge, and improve over time. The platform can estimate complication risk, ICU admission probability, readmission risk, or extended length of stay while keeping medical decisions under human control.
Computools’ web development services support the user-facing side of the platform: surgeon dashboards, anesthesiologist views, coordinator worklists, executive analytics, admin panels, and role-specific alerts. These interfaces turn clinical data analytics into daily decisions instead of static reports.
For hospitals, this service mix addresses the key challenge concerning predictive surgical risk software: integrating data, AI, workflows, integrations, and security within a single decision-support framework. This offers earlier visibility of risks, and with less need for manual interventions, more robust coordination of perioperative activities is achieved alongside safe and flexible data handling. All these support scaling with new models, new departments, and new clinical workflows.
Final thoughts
To gain the real value from surgical risk prediction software, hospitals must view this software as an operational decision-support system. The solution must offer an integrated environment for the EHR, clinical data, perioperative workflows, risk models, alerts, audit trails, and secure user access.
The strongest results come when data, AI, and workflow design move together. Clean clinical data improves prediction quality. Secure EHR integration keeps risk scores current. Explainable AI builds clinician trust. Workflow automation routes high-risk cases to the right team before delays, complications, or resource pressure increase.
For hospital administrators, the business case is simple. There is earlier patient risk stratification, fewer hand calculations, improved coordination and planning, as well as reduced burdens and better surgical service line capacity. The platform improves availability and focus of clinical line staff and provides executives the data to manage performance, risk, and resources effectively.
Computools
Software Solutions
Computools is an IT consulting and software development company that delivers innovative solutions to help businesses unlock tomorrow.






