THE AUTHOR:

Why are companies looking to develop an ICSR processing system in 2026? They need a controlled drug safety operations platform that can capture adverse event reports, validate minimum case criteria, structure source data, support medical review, and prepare cases for electronic submission.
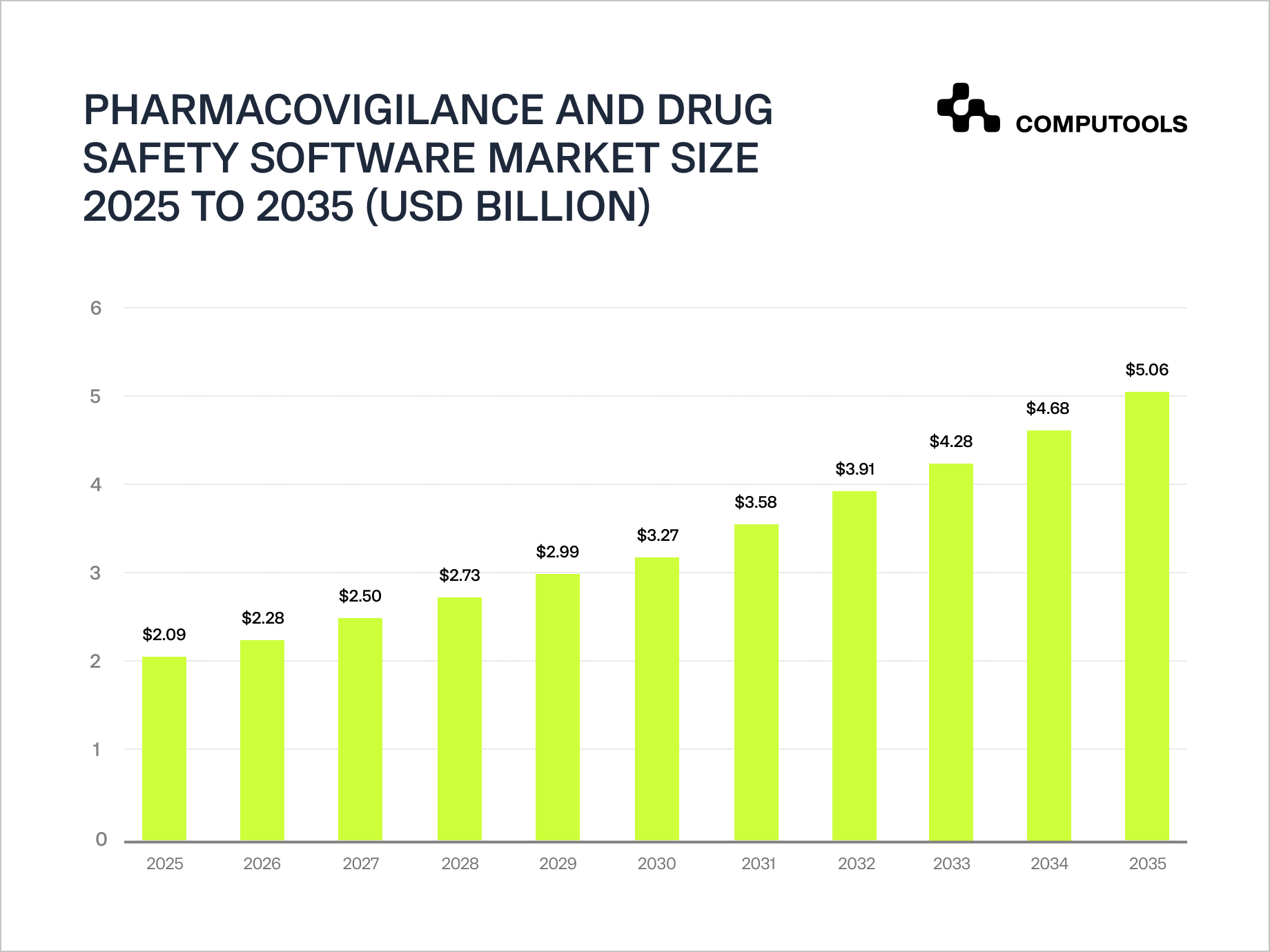
The pressure is building on safety reporting. Safety data are now scattered across emails, PDFs, call centers, patient support programs, partner portals, medical literature, and global affiliates. Automation is now a key element across all safety reporting. The value of the global pharmacovigilance and drug safety software market was USD 2.09 billion in 2025, and is expected to reach USD 5.06 billion by 2035, signifying a positive industry shift towards automation, workflow control, data- and evidence-based safety reporting and oversight.
Regulators are moving safety reporting toward newer electronic formats. In the U.S., FDA now requires some IND safety reports submitted through ESG NextGen to follow the E2B(R3) standard, and from October 1, 2026, this format will apply to all ICSRs submitted to AEMS through ESG NextGen. In the EU, EMA already requires ICSR submissions to EudraVigilance in the ISO ICSR / ICH E2B(R3) format and no longer accepts the older E2B(R2) format.
An automated ICSR management system is now responsible for a wide spectrum of tasks including: case intake, validity checks, duplicate detection, MedDRA, and WHODrug coding support, narrative generation, SLA tracking, quality review, E2B(R3) mapping, and audit ready case history. Although AI has the potential to significantly decrease manual effort related to extraction, triage, coding, follow-up detection, and drafting narratives, it has to work with clean data and requires reviewer’s judgement, validation, and clear accountability.
This article shows how to develop an ICSR processing system that incorporates automation, structured safety data, a human medical review, regulatory compliance, integrations with safety databases, and the ability to monitor the performance of drug safety operations after product launch, all in a single scalable platform.
Core features of an automated ICSR processing system
Each function of drug safety operations software should reduce a specific risk: slow intake, incomplete case data, missed deadlines, duplicate reports, inconsistent coding, weak audit trails, or poor visibility across drug safety teams.
| Feature | What it should do | Business value |
| Multi-channel case intake | Capture safety reports from emails, PDFs, portals, web forms, call center notes, partner systems, and literature workflows. | Reduces fragmented reporting and gives PV teams one controlled intake point. |
| OCR and NLP extraction | Read unstructured and scanned documents, extract patient, reporter, product, event, dates, dosage, outcome, and source details. | Cuts manual data entry and moves cases to review faster. |
| Case validity checks | Check whether the report contains an identifiable patient, identifiable reporter, suspect product, and adverse event. | Prevents non-valid reports from entering regulated case workflows too early. |
| Duplicate detection | Compare new reports against existing cases using product, patient, event, date, reporter, and source patterns. | Protects case quality and prevents inflated safety counts. |
| MedDRA and WHODrug coding support | Suggest standardized medical terms and drug dictionary matches for reviewer approval. | Improves consistency and reduces coding workload. |
| SLA and deadline tracking | Track reporting timelines by case seriousness, market, product, sponsor, and workflow status. | Gives managers early visibility into deadline risk. |
| Human review workspace | Show extracted data, source evidence, AI suggestions, reviewer edits, comments, and case history in one place. | Keeps expert review efficient, traceable, and accountable. |
| Narrative drafting | Generate editable case narratives from structured fields and source documents. | Reduces repetitive writing while keeping final control with reviewers. |
| E2B(R3) mapping and validation | Prepare structured case data for electronic exchange with safety databases or regulatory systems. | Reduces late-stage formatting issues and submission errors. |
| Integration layer | Connect with Argus, ARISg, Veeva Vault Safety, email systems, document repositories, and regulatory gateways. | Prevents duplicate data entry and keeps safety operations connected. |
| Audit trails and electronic signatures | Record user actions, field changes, approvals, timestamps, previous values, and final case versions. | Supports inspection readiness and controlled compliance workflows. |
| Analytics dashboard | Show workload, backlog, case aging, automation rate, correction rate, SLA risk, and submission performance. | Turns drug safety operations into a measurable management system. |
The strongest platforms combine these features into one controlled workflow. Intake automation should feed structured data into review. Review should feed correction data back into AI improvement. Submissions should connect with acknowledgment tracking. Dashboards should show where work is slowing down before deadlines are missed.
This is also where the business case becomes clearer. A well-designed platform does not only reduce manual processing time. It gives safety leaders better control over capacity, quality, compliance risk, and operational scalability.
Computools case study: how to develop an ICSR processing system
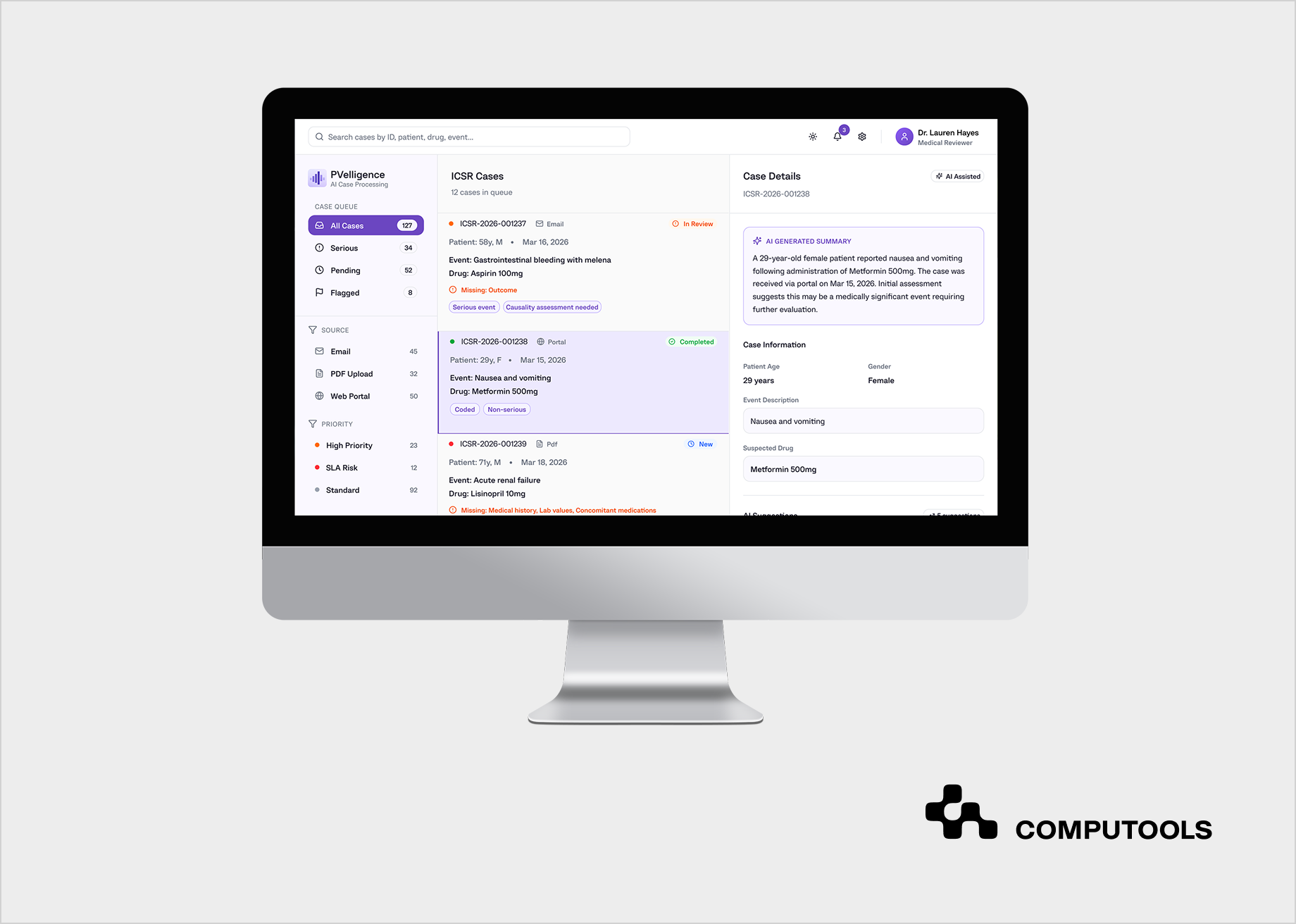
Consider the example of PVelligence, the AI-based pharmacovigilance automation platform. Computools developed it for a contract research organization managing high-volume drug safety operations for multiple life sciences sponsors. The client processed thousands of ICSRs every month. The case safety reports came from disparate sources that included emails, PDFs, portal submissions, and semi-structured safety submissions. As case volume increased, routine work around intake, validation, MedDRA coding, WHO-DD mapping, narrative drafting, and regulatory preparation became a direct operational bottleneck.
In addition, the CRO had to manage different sponsor SOPs, reporting priorities, review expectations, and compliance requirements inside one operating environment. Existing safety systems could store and process cases, but they did not reduce the manual work enough at the front of the workflow. Serious cases still needed faster triage, reviewers needed cleaner structured data, and managers needed better visibility into workload, bottlenecks, and SLA exposure.
Computools designed PVelligence as a two-layer platform: ICSR workflow automation and medical review augmentation. The first layer automated intake, data extraction, structuring, validity checks, triage, coding support, automatic case creation in safety systems, narrative drafting, and regulatory output preparation.
The second layer supported physicians and PV specialists with AI-generated pre-assessments for seriousness, expectedness, causality cues, and reporting suggestions, while final medical and regulatory decisions stayed under expert control.
Technically, the platform used Python for data processing pipelines, integration logic, and AI model execution. NLP and LLM models extracted structured safety data from unstructured emails, PDFs, and web forms, identifying core ICSR elements such as patient, reporter, suspect drug, and adverse event. Machine learning supported triage, seriousness classification, prioritization, and early pattern analysis. RPA automated repetitive actions such as case creation in safety systems and regulatory document preparation. The integration layer connected the platform with pharmacovigilance systems such as Oracle Argus and ARISg, as well as email systems and document repositories.
The result was measurable operational improvement. Case preparation time dropped from 4–6 hours to 10–20 minutes before final human review. Up to 60–70% of manual processing effort was automated across intake, structuring, coding, and narrative preparation. The client gained faster medical review, clearer workflow visibility, stronger SLA control.
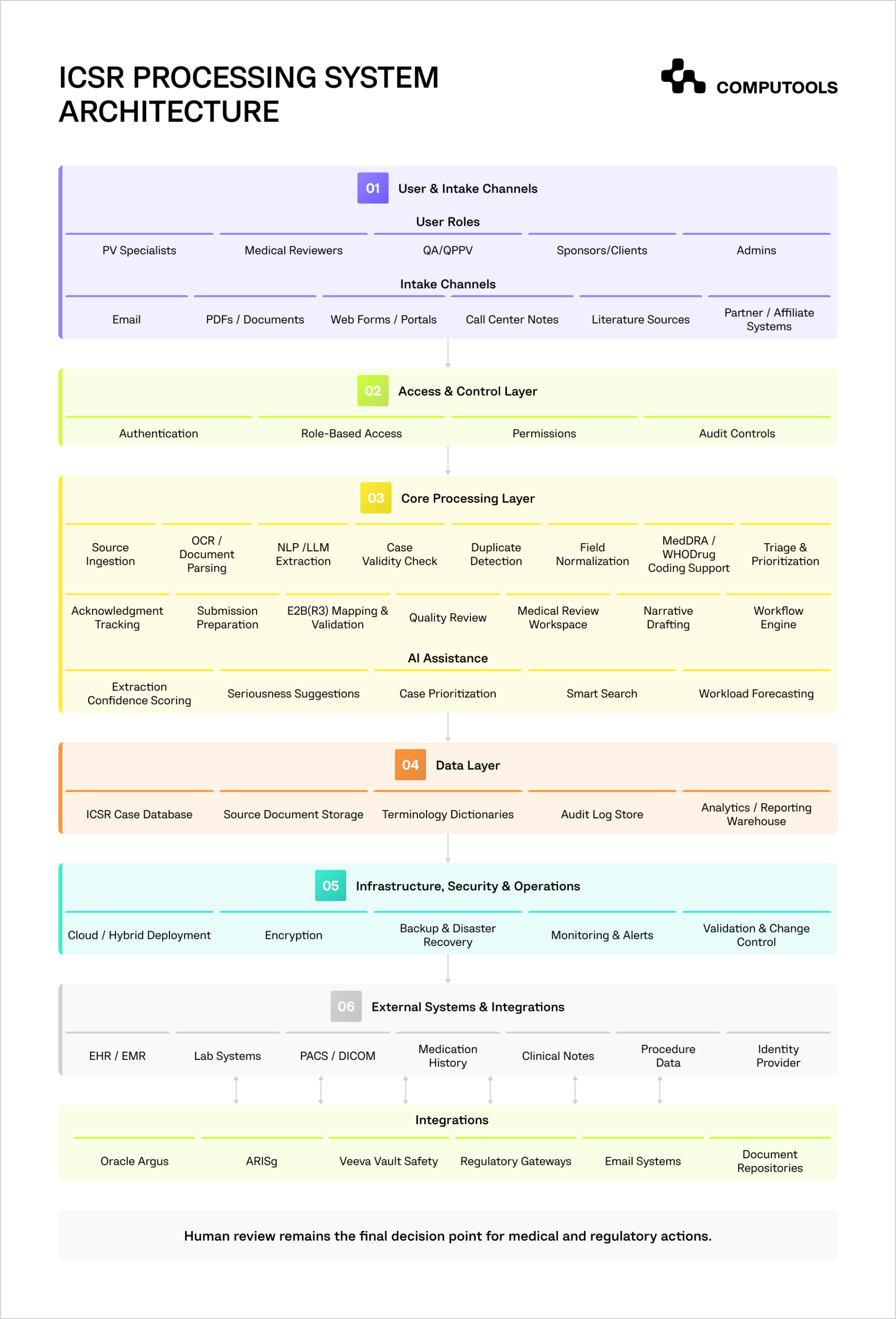
The same logic applies to any company planning to develop an ICSR processing system: the architecture must connect intake, structured data, validation, AI support, human review, regulatory preparation, integrations, and audit control from the start.
Develop an ICSR processing system: a step-by-step guide
An ICSR platform should collect fragmented reports, validate minimum case criteria, structure safety data, support expert review, prepare regulatory outputs, and keep every action traceable. For ICSR software development, the main question is “Which operational risks should the system control before case volume, reporting timelines, and data quality become harder to manage?”
1. Define the pharmacovigilance operating model first
Before development starts, the business should define how cases enter the organization, who reviews them, which markets the company reports to, and which safety systems remain in use.
This process is important because adverse event case processing typically involves multiple teams, including but not limited to intake specialists, case processors, medical reviewers, quality reviewers, regulatory teams, QPPV teams, sponsors, and system administrators.
The operating model should encompass case sources such as email, PDF, web forms, case report portals, notes from call center interactions, and documentation from patient support programs and partner systems as well as outputs from literature monitoring. The model should also describe how the system manages spontaneous case reports, solicited reports, follow-up reports, duplicate reports, exceptional cases, serious adverse events, and invalid case reports.
From a technical standpoint, this requires configurable case management. The system should provide the ability to define and implement configurable business rules for different sponsors, products and markets, case types, languages, and case reporting timeframes. Ignoring this requirement may lead to a system design that is optimal for one team, while fundamentally failing to meet the needs of supporting a different sponsor, country, product, or standard operating procedure (SOP).
A practical design starts with a workflow map:
intake → validity check → duplicate check → triage → coding support → case processing → medical review → quality review → regulatory preparation → submission or safety system transfer → acknowledgment tracking.
This map becomes the foundation for user permissions, SLA timers, dashboards, audit trails, and automation logic.
2. Build the ICSR data model around E2B(R3) requirements
The data model is crucial for safety case processing software. It should address internal workflow and regulatory exchange from the outset. The FDA will require all individual case safety reports (ICSRs) submitted via the FDA’s Electronic Submission Gateway (ESG) to the FDA’s AEMS system to conform to E2B(R3) data standards by October 1, 2026. The European Medicines Agency (EMA) requires reports to EudraVigilance to conform to the ISO ICSR / ICH E2B(R3) format.
The data model should include all core ICSR components inclusive of the patient, reporter, suspected and concomitant products, adverse event, criteria for seriousness, outcome, and elements of the exposure (dosage, route and indication), and elements of the medical history and lab data, as well as narrative and source data, the follow-up edition, and the regulatory destination. It should also address controlled vocabularies for MedDRA, WHODrug, ISO country codes, and pharmaceutical forms and routes of administration.
The technical logic should connect each structured field to its source evidence. For instance, if a suspect product is extracted from a PDF using AI, the system must store the original document, extracted information, source text, confidence level, corrections made by the reviewer, date and time of the correction, and final approved value. This facilitates medical review and audit validation of the case.
A weak data model creates long-term problems. Teams may need to re-enter data into Argus, ARISg, Veeva, or another safety database. E2B mapping becomes harder. AI extraction becomes less reliable. Reporting teams lose time fixing data instead of preparing cases for submission.
3. Automate intake, extraction, and case validity checks
The first area of focus for automation should be intake. This is the area that causes the most time loss for drug safety teams. Reports come in varied formats. They also may be duplicated and include information that is incomplete or poorly structured. The platform must be able to transform these inputs into structured case records while still providing case management control to experts.
A functional intake pipeline must be able to do source ingestion, file type identification, OCR for scanned documents, extraction using NLP or LLM, mapping, confidence scoring, basic case validation, duplicate identification, and target review queue placement. The system must determine and identify the four basic criteria of validity. An identifiable patient and reporter, alongside the suspect product and adverse event, must all be present.
In the PVelligence project, Computools used NLP and LLM models to extract safety data from unstructured emails, PDFs, and web forms, including patient, reporter, suspect drug, and adverse event details. The same logic is critical for companies building an automated ICSR processing system because the highest workload often starts before the case reaches the safety database.
The platform should not auto-approve uncertain data. Low-confidence fields should move to a reviewer queue with the source evidence displayed next to the extracted value. This keeps automation useful without turning it into an uncontrolled risk.
Computools’ article on how to build an AI system for clinical documentation gives a useful parallel for ICSR platforms that use AI to prepare case narratives and extract safety data from clinical text.
4. Design configurable workflows for case processing and review
Pharmacovigilance case management software requires more than simple task assignment. It should manage the entire lifecycle of a case including should manage the entire lifecycle of a case including case status, definition of required fields, available actions for case reviewers, case escalations, the timers for SLA, and the built-in quality check features.
The team should determine which rules are fixed and which ones can be configured. For instance, a serious case might require the review to be expedited along with a medical review and stricter review escalations. Alternatively, a non-serious follow-up case will have a different review process. It is also possible that a contract research organization may require sponsor-related rules within the same case management system.
From a technical perspective, the workflow layer should address case status, permissions based on role, case review task queues, task assignment rules, case escalations, deadlines, comments, version control, and the log of audit records.
If this step is ignored, teams will keep using spreadsheets to track deadlines and emails to chase missing actions. The platform may store cases, but it will not reduce operational pressure.
5. Connect the platform with safety systems and regulatory reporting channels
Most organizations already use safety databases, document repositories, email systems, medical information systems, or partner portals. The ICSR platform should connect with this wider environment instead of creating another isolated tool.
The business should decide whether the new system will replace part of the current workflow, extend an existing safety database, or act as an automation layer before cases move into systems such as Oracle Argus, ARISg, or Veeva Vault Safety. This decision affects architecture, integrations, validation scope, and user adoption.
The technical layer should support APIs, secure file exchange, message queues, retry logic, error dashboards, reconciliation logs, and acknowledgment handling. The ICH E2B(R3) implementation guide defines data elements and message specifications for electronic ICSR transmission, so the system should be designed with structured mapping and validation rather than late-stage export fixes.
In PVelligence, Computools built an integration layer for pharmacovigilance systems such as Oracle Argus and ARISg, plus intake sources such as email systems and document repositories. This matters because ICSR automation only creates business value when extracted and reviewed data can move into the systems where regulatory work actually happens.
6. Add AI where it reduces workload and keeps expert review in control
AI for ICSR processing should focus on repetitive, evidence-based tasks. Some prominent examples include classification of intake, entity extraction, duplicate identification, seriousness assessment and prioritization, coding, detection of follow-ups, construction of narratives, and even workload prediction.
Each application of AI should serve a distinct business goal. Duplicate detection protects case quality and signal analysis. Narrative drafting reduces writing time. Smart search lets reviewers compare similar cases faster. Priority scoring moves serious cases to the front of the queue. Predictive analytics can show which teams, sponsors, products, or intake channels are likely to create SLA risk.
The system should also show how AI reached a suggestion. Reviewers need to see the supporting evidence, assess AI’s confidence, review the version history, and either accept, modify, or deny the recommendations. Artificial intelligence relies on accurate structured data, so part of the data strategy should include historical case quality, reviewer corrections, and terminology consistency.
The principal concern is the risk of over-automation. In the absence of proper review controls, the output of AI moving through the workflow will actually result in an increase of quality risk for the organization, as opposed to the intended reduction of workload. The less risky approach is to allow qualified professionals to finalize medical and regulatory decisions, and allow AI to prepare, prioritize, and perform ancillary checking tasks.
If the platform uses AI for extraction, duplicate detection, triage, or narrative drafting, the architecture should separate model logic from regulated approvals. Computools explains this approach in its guide on HIPAA-compliant AI architecture.
7. Build compliance, security, and audit readiness into the architecture
Regulatory compliance software for pharmacovigilance should always protect patient privacy, maintain the integrity of the case, and keep the organization inspection ready at any time. While security compliance is an important checklist item, absence of security measures affects trust and continuity, and impacts sponsor confidence. Additionally, the inability to demonstrate safety data compliance in the correct manner also impacts the business.
The system must include role-based access, encryption, secure authentication, e-signatures if applicable, audit trails, permanent backups and recovery, retention policies, validated change control, and record the identity, time, and reason for the change, as well as the previous value and the new value.
For regulated workflows, audit trails should cover the entire lifecycle of the submission and all actions taken within the system either directly or as a result of an AI suggestion. It should cover intake, extraction, reviewer edits, AI suggestions, coding changes, narrative updates, status changes, submission preparation, and integrations. If the system cannot explain how a final case version was created, it becomes risky during inspections and quality reviews.
This step should start during software architecture design. If audit controls, permissions, and validation evidence are added late, the team may need to redesign core workflows after development.
ICSR platforms often run in cloud or hybrid environments, so security should be planned around PHI protection, access control, encryption, audit logging, backup, and recovery.
Computools covers these controls in more detail in its article on cloud security in healthcare businesses, which is relevant for pharmacovigilance software solutions that store sensitive patient and reporter data.
8. Test with real case complexity before launch
Testing should reflect real pharmacovigilance operations, not only clean demo scenarios. The platform should be tested with incomplete reports, duplicate cases, scanned PDFs, multilingual documents, follow-up versions, serious cases, non-valid reports, conflicting dates, missing reporter information, and sponsor-specific SOP variations.
The testing strategy involves a number of different approaches. Primarily the strategy outlines the need for functional testing, integration testing, security testing, validation testing, user acceptance testing, and extraction accuracy checks. It should include load testing, E2B(R3) validation, regression, and audit trail review testing. It should also account for failures due to integration issues, failures due to a rejection of regulatory acknowledgement, and failures due to an AI confidence drop below the acceptance threshold.
Post-launch, the operational key performance indicators (KPIs) of the platform will be the measurement of case preparation time, automation rate, reviewer correction rate, breaches of the service level agreement (SLA), quality of duplicate detection, submission error rate, backlog size, queue aging, and the cost per processed case.
This is where ICSR automation becomes a managed business system rather than a one-time software release. The platform should keep improving as source documents change, case volumes grow, sponsor rules shift, and AI models receive better correction data from reviewers.
Launch your production-ready ICSR automation platform within 1–3 months instead of years, and start processing more safety cases without expanding your pharmacovigilance team.
Why choose Computools to develop an ICSR processing system
At Computools, we see the development of an ICSR platform as part of a larger operational transformation, rather than an isolated software development effort. Drug safety teams face a growing gap between case volume, manual review capacity, regulatory timelines, data quality, and the number of systems involved in pharmacovigilance work.
This is the challenge that Computools aims to solve as a technology partner. We align the product architecture with the broader business system that includes the safety data systems, workflows, sponsor requirements, compliance systems, and performance metrics. The design intent is to minimize processing friction and keep medical review, data traceability, and regulatory accountability under control.
Computools’ work on PVelligence shows this approach in practice. The platform integrated AI-based data extraction, ICSR process automation, medical review, regulatory readiness, and systems support for pharmacovigilance such as Oracle Argus and ARISg. The system provided PV teams with more structured data that facilitated the final review, and, instead of eliminating the need for expert judgment, lessened the burden of repetitive work.
For companies planning similar platforms and custom pharmacovigilance software, Computools healthcare software development services can support the full delivery path. Our expertise is relevant for systems that handle sensitive patient data, regulated workflows, audit trails, and secure user access. Our hospital software development services add experience with clinical workflows, healthcare integrations, protected records, and role-based environments. Through web development services, Computools can build reviewer portals, sponsor workspaces, admin panels, and operational dashboards that make complex safety work easier to control.
The technical foundation also matters. With AI development, we design extraction, duplicate detection, triage, smart search, narrative drafting, and reviewer assistance features with clear approval logic. With data engineering, the team can structure safety data pipelines, terminology mapping, analytics layers, integration flows, and reporting foundations needed for long-term automation.
A strong ICSR platform should not force the business to choose between speed and control. Computools designs systems that automate routine work, connect with existing safety infrastructure, protect regulated data, and give operations leaders better visibility into case flow, SLA risk, reviewer workload, and compliance readiness.
Computools is also listed among the top healthtech software development companies, which supports its positioning for regulated healthcare and pharmaceutical software development services.
Final thoughts
An ICSR processing system should have the capability to manage how adverse event data enters the organization, how it is structured, how reviewers verify it, how regulatory outputs are generated, and how management monitors workload, quality, and risk of SLA breaches.
If companies choose to develop an ICSR processing system with this broader perspective, they enjoy benefits that include shortened time for case preparation, reduction in repetitive manual tasks, increased data consistency, maintenance of audit readiness, unification of disparate pharmacovigilance processes, and increased scalability for drug safety operations.
The most advanced systems integrate structured data with configurable workflows, AI-assisted processing, and human medical review, along with secure integrations and E2B(R3) readiness and offer a proactive approach to performance. Drug safety workflow automation is most effective when it enhances rather than undermines expert control.
Computools
Software Solutions
Computools is an IT consulting and software development company that delivers innovative solutions to help businesses unlock tomorrow.






